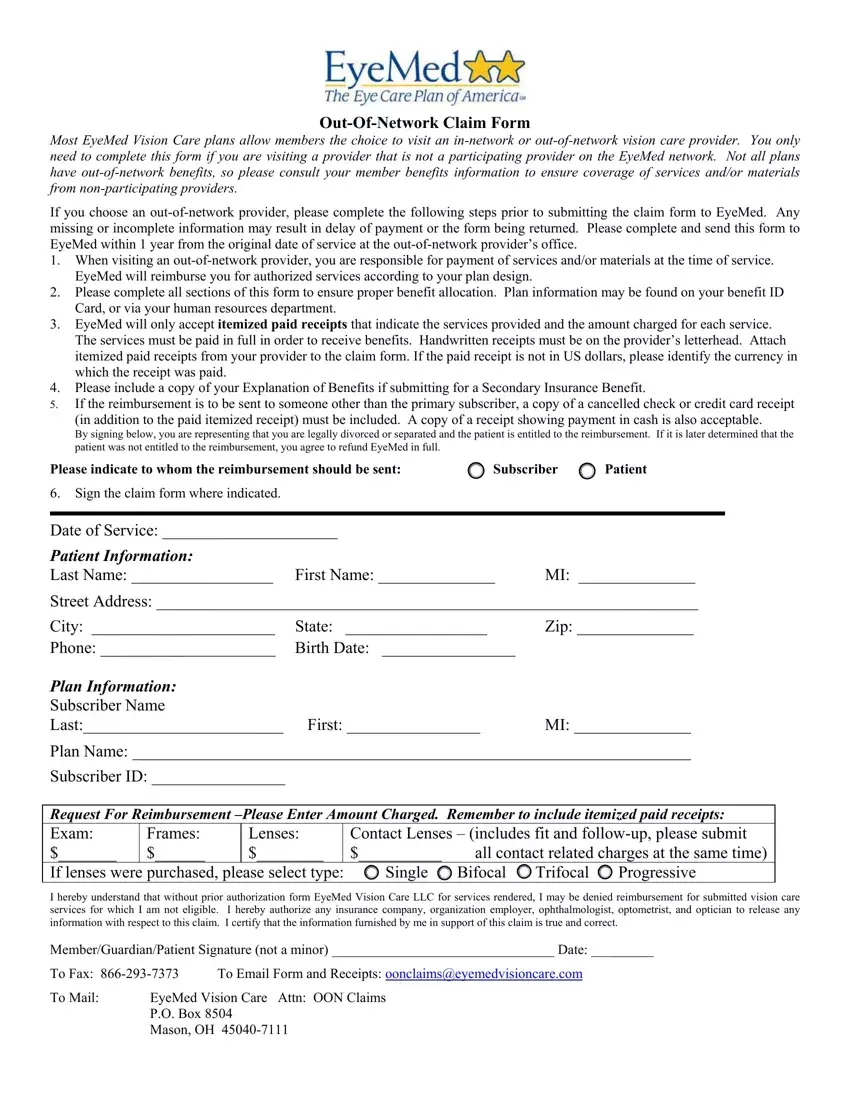
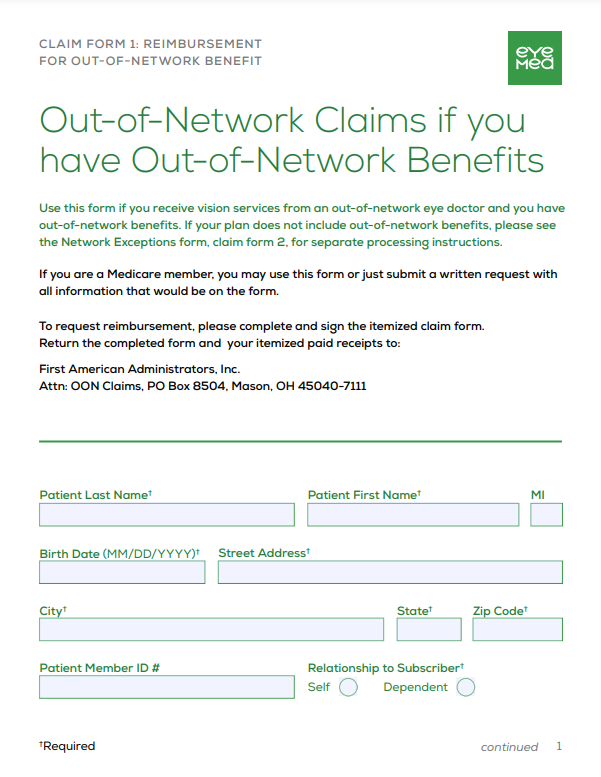
Eyemed Out Of Network Form - To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. To request reimbursement, please complete and sign the. You will need patient, subscriber, doctor or store information. One of the following exceptions must. If your plan does not.
If your plan does not. One of the following exceptions must. You will need patient, subscriber, doctor or store information. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours.
To request reimbursement, please complete and sign the. One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. If your plan does not. You will need patient, subscriber, doctor or store information.

EyeMed Reimbursement 9FIVE Eyewear
If your plan does not. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. One of the following exceptions must. You will need patient, subscriber, doctor or store information.

Fillable Online Eyemed Claim Form Fill Out and Sign Printable PDF
One of the following exceptions must. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. You will need patient, subscriber, doctor or store information. If your plan does not.
Eyemed Claim Form Printable Printable Forms Free Online
To request reimbursement, please complete and sign the. If your plan does not. One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. You will need patient, subscriber, doctor or store information.

Insurance Pdf 44016 Fsl S Access Plan For The Eyemed Select Network Data
If your plan does not. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. One of the following exceptions must. You will need patient, subscriber, doctor or store information.

Fillable Online EyeMed Claim Form Yumpu Fax Email
You will need patient, subscriber, doctor or store information. If your plan does not. To request reimbursement, please complete and sign the. One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours.

EyeMed_Enrollment_Form Keyser Insurance Group
One of the following exceptions must. If your plan does not. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. You will need patient, subscriber, doctor or store information.

Eyemed Insurance Out Of Network Claim Form Creativmakeup Co
One of the following exceptions must. You will need patient, subscriber, doctor or store information. If your plan does not. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. To request reimbursement, please complete and sign the.
EyeMed Reimbursement Form
One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. If your plan does not. You will need patient, subscriber, doctor or store information. To request reimbursement, please complete and sign the.
Eyemed Medically Necessary PDF Form FormsPal
One of the following exceptions must. To request reimbursement, please complete and sign the. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. You will need patient, subscriber, doctor or store information. If your plan does not.
Fillable Online claim submissions made easy EyeMed Fax
One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours. If your plan does not. You will need patient, subscriber, doctor or store information. To request reimbursement, please complete and sign the.
To Request Reimbursement, Please Complete And Sign The.
If your plan does not. You will need patient, subscriber, doctor or store information. One of the following exceptions must. To submit a claim please enter your email address below and we'll email you a link that will only be active for 24 hours.