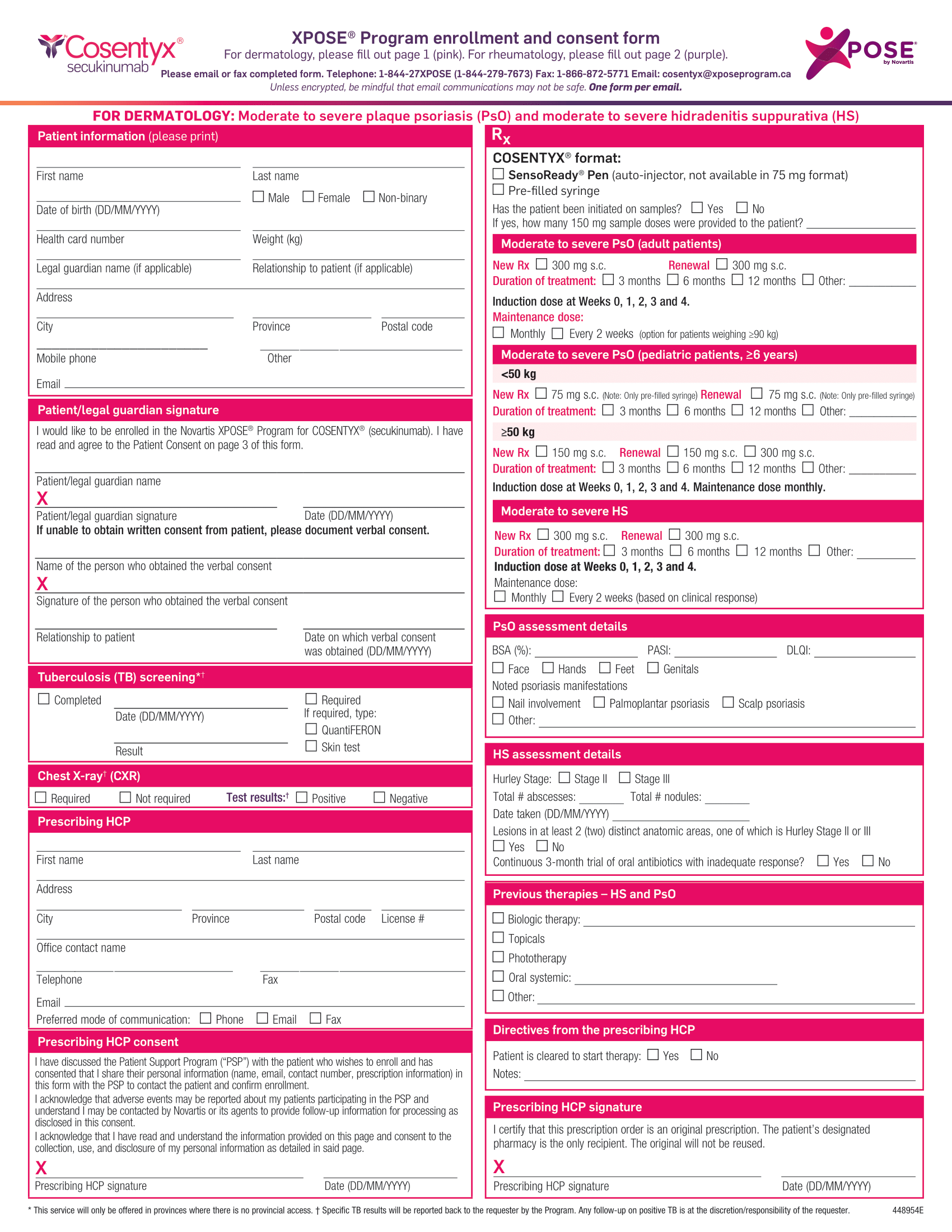
Cosentyx Enrollment Form - Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are.
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
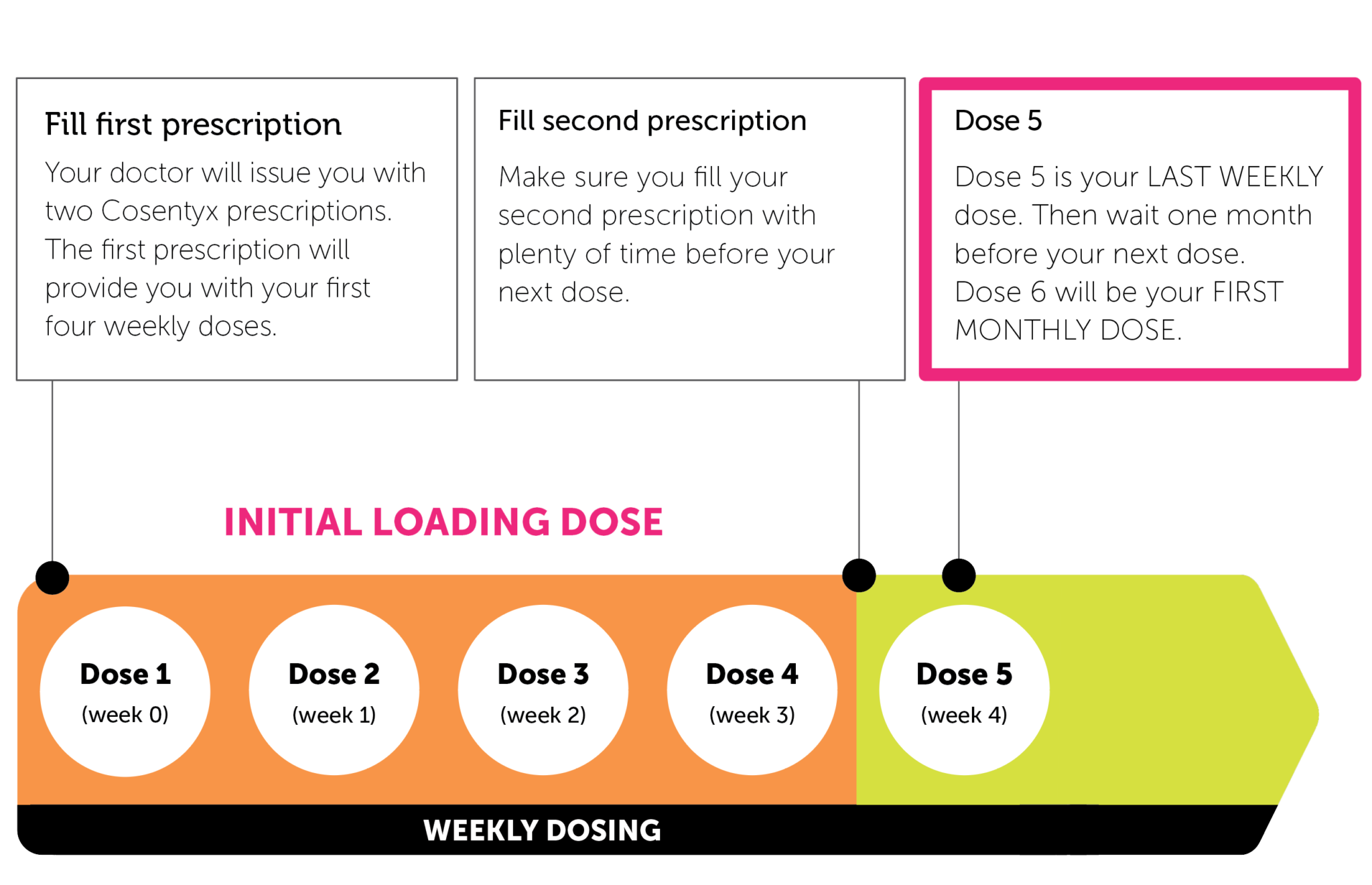
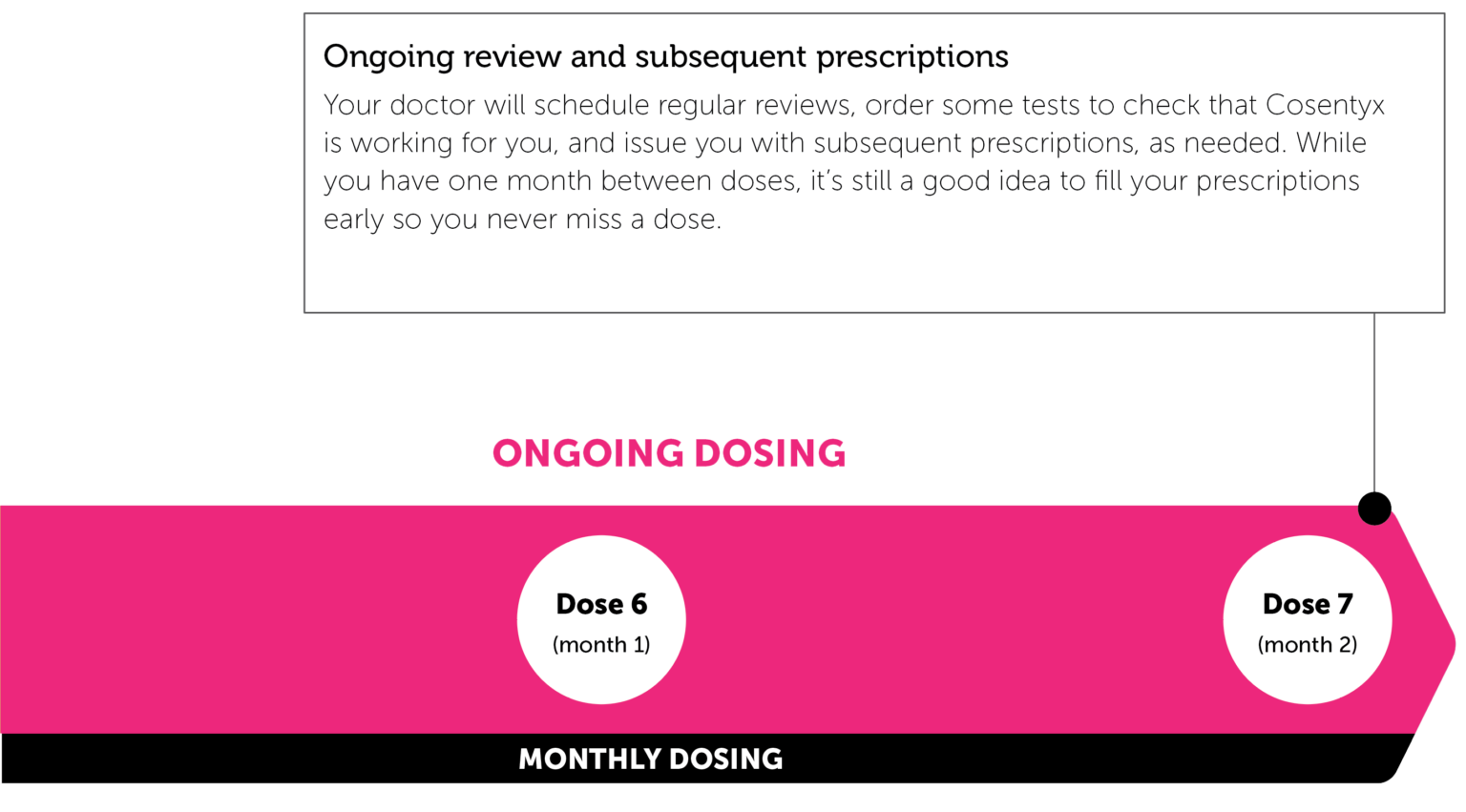
Speak to your nurse or doctor if you do not know your dose or are
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
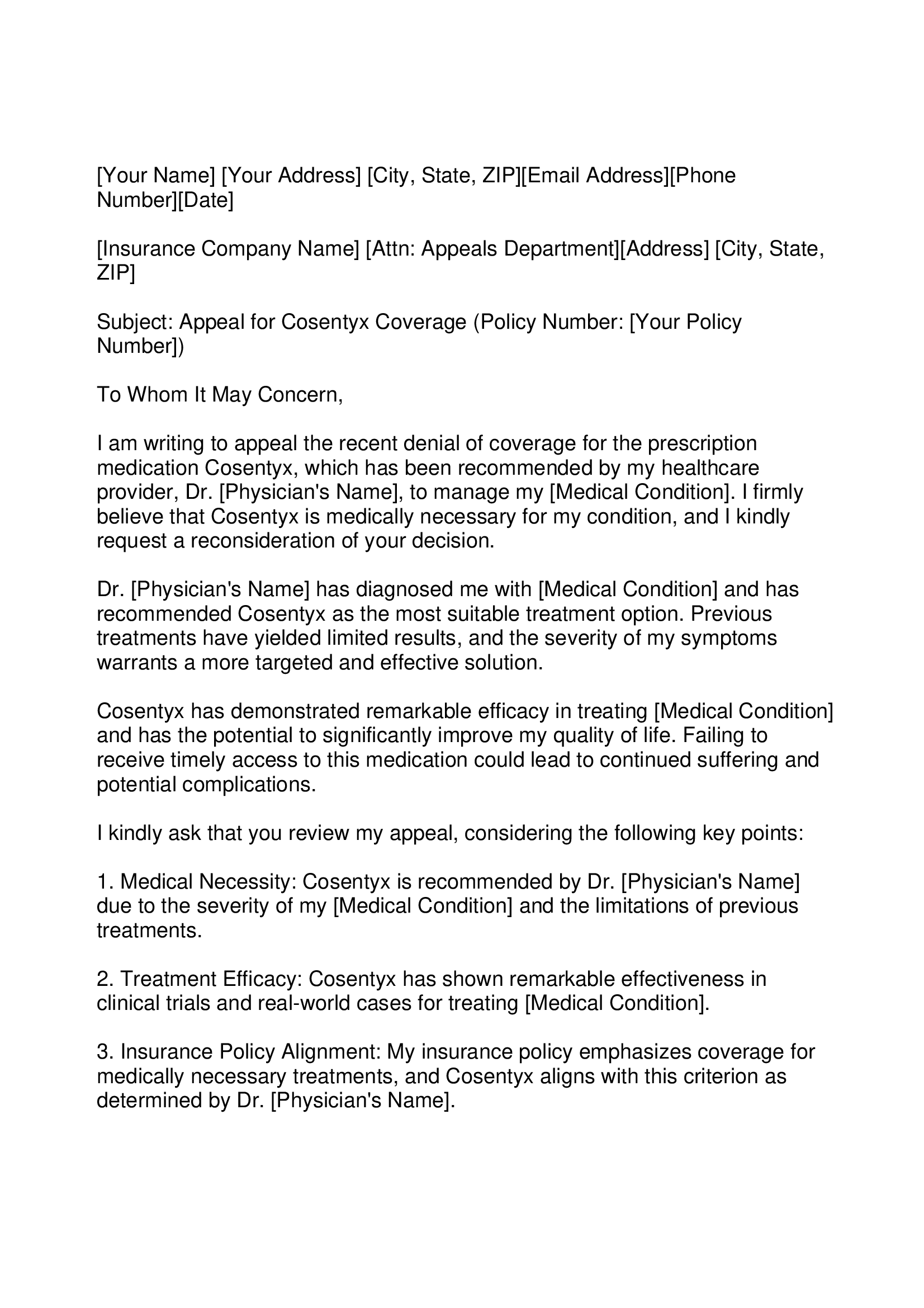
Cosentyx Appeal Letter Forms Docs 2023
Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
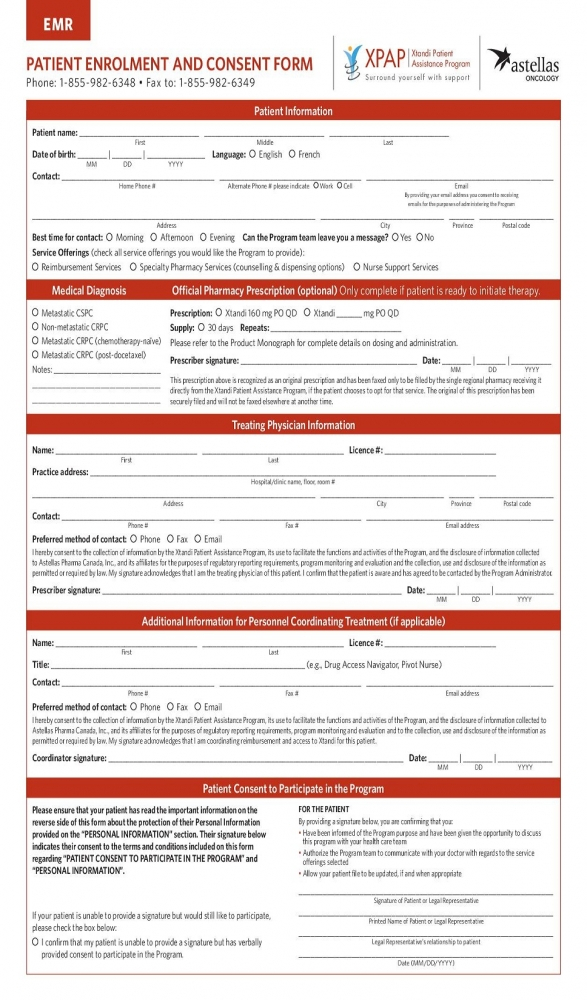
Xtandi Support Solutions Patient Enrollment Form Enrollment Form
Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.

Cosentyx FDA prescribing information, side effects and uses
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.

MedicinesRheumatology Novartis Ireland HCP Portal
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
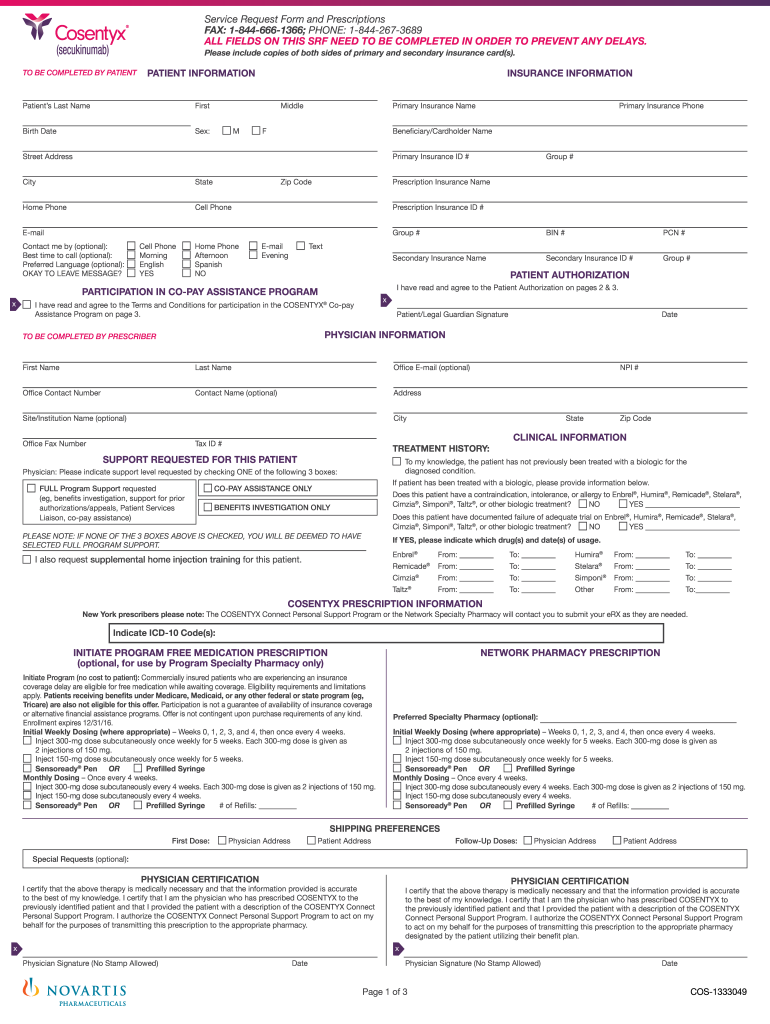
Cosentyx Enrollment Form 2023 Printable Forms Free Online
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
Cosentyx Injection 150 mg 3S Corporation Pharmacy & Drugs Dealers
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
Xelsource Enrollment Form Pdf Enrollment Form
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.
Not an Altogether You member? Find out what Altogether You has to offer
Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are.
Cosentyx (secukinumab) PSP Enrollment Form 2024 The Oscar Galaxy
Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous. Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are.
Start Form (Mm/Dd/Yyyy) *The Covered Until You’re Covered Program Is Available For Cosentyx® (Secukinumab) Subcutaneous.
Cosentyx ® (secukinumab) is indicated for the treatment of moderate to severe plaque psoriasis (pso) in patients 6 years and older who are. Start form (mm/dd/yyyy) *the covered until you’re covered program is available for cosentyx® (secukinumab) subcutaneous.